There are many different treatment options available to people with Waldenstrom macroglobulinemia (WM). If you’re having WM-related symptoms that require treatment, your hematologist/oncologist will recommend a treatment plan tailored to your specific medical situation.
What factors are important when developing a treatment plan?
There are a number of recommended therapy regimens that are appropriate choices for treating WM. Your hematologist/oncologist will take several factors into account when deciding what regimen is best for you, including:
-
- Your age
- Your general health and quality of life
- The type and extent of your symptoms
- Blood, bone marrow, and other test results
- The need for rapid disease control
- Any previous treatments you’ve had to manage your WM
- Your eligibility and possible need for a stem cell transplant now or in the future
What therapy regimens are used to treat WM?
The medications used to treat Waldenstrom macroglobulinemia can be given is a variety of combination and schedules. Most of the recommended regimens include rituximab (Rituxan®) and one or more chemotherapy drugs.
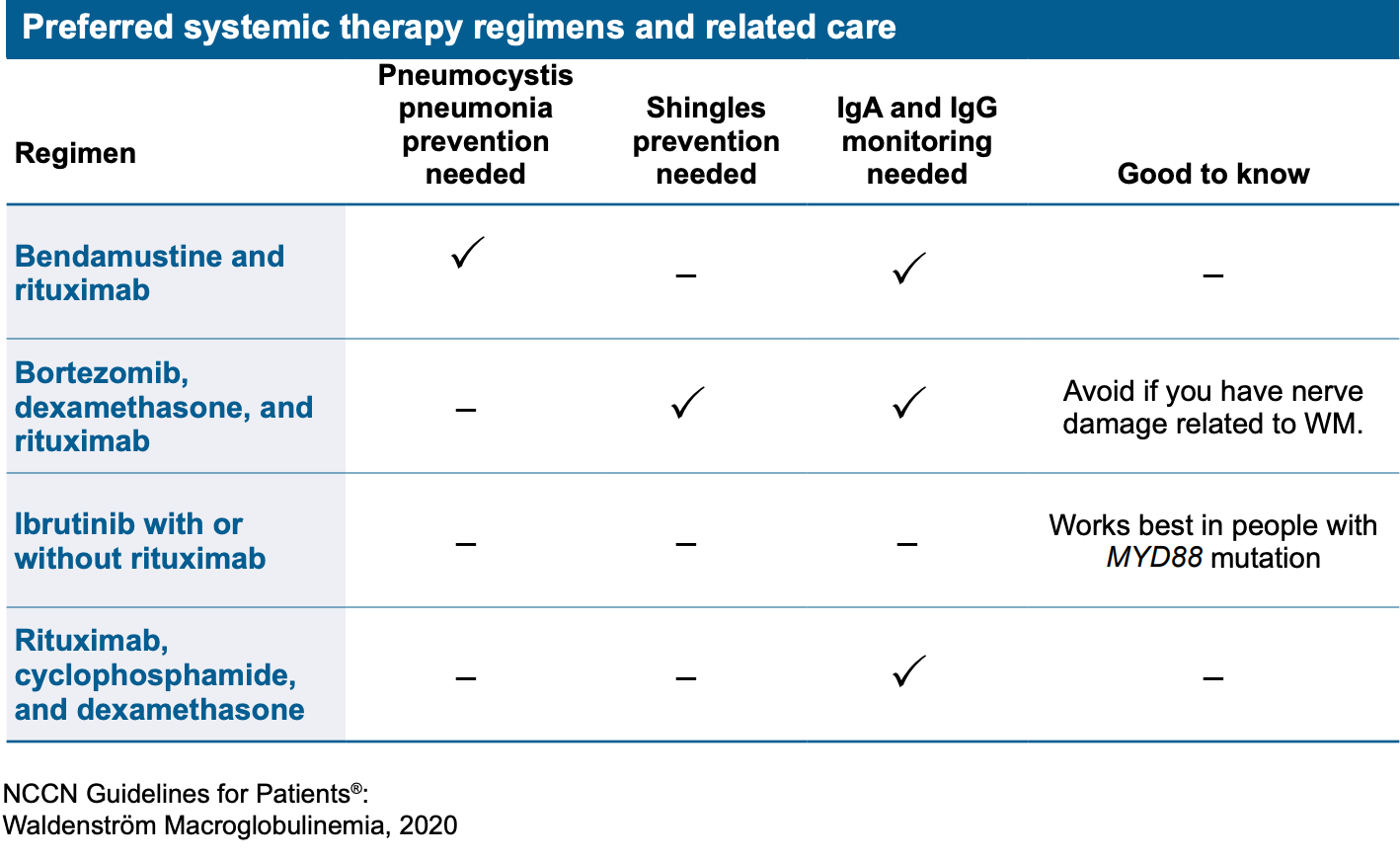
There are four first-line therapy regimens currently preferred by both the WM experts of the National Comprehensive Cancer Network (NCCN) – an alliance of 30 leading cancer centers in the U.S. – and the international consensus panel of WM experts who participated at the tenth International Workshop for Waldenstrom Macroglobulinemia (IWWM-10). These two groups of world-renowned WM experts develop treatment recommendations that are regularly updated to reflect the most current data available. The four preferred regimens are outlined in the following chart; they are listed alphabetically.
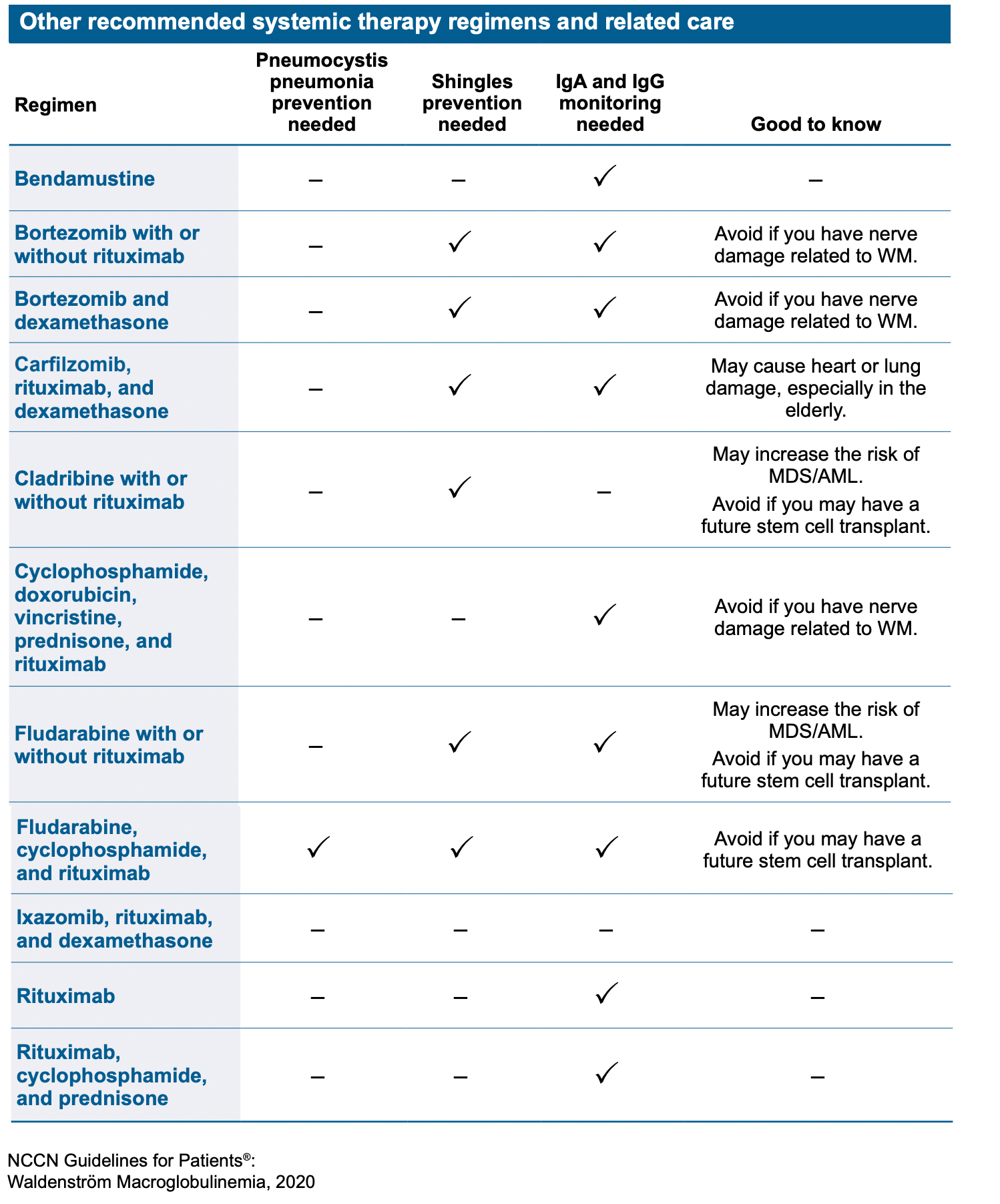
 While the four therapy regimens listed above are preferred, there are many other regimens that are recommended for treatment as well. The choice of therapy should be guided by your clinical profile; any genetic mutations identified (for example, mutations in the MYD88 or CXCR4 genes); and drug availability.
While the four therapy regimens listed above are preferred, there are many other regimens that are recommended for treatment as well. The choice of therapy should be guided by your clinical profile; any genetic mutations identified (for example, mutations in the MYD88 or CXCR4 genes); and drug availability.
What related care should be considered when receiving treatment for WM?
As noted in the previous two charts, some treatment regimens call for related medical care. This includes the prevention of shingles and pneumocystis pneumonia, and making sure the levels of two antibodies, IgA and IgG, don’t get too low. Additional blood tests will be taken at intervals to prevent other side effects of treatment.
- Shingles: This is a painful skin rash caused by the same virus that causes chicken pox. Some treatment medications can reactivate shingles. To reduce this risk, your doctor may recommend you get the shingles vaccine and/or take the antiviral medicine acyclovir (Zovirax®) or valacyclovir (Valtrex®) before starting treatment.
- Pneumocystis jiroveci pneumonia (PJP): This is a fungal infection of the lungs, most often seen in people with a weak immune system. Your doctor may order a medication to lower the risk of PJP when using certain therapy regimens.
- IgA and IgG monitoring: Many treatment medications can cause the levels of IgA and IgG to become low. Blood tests are used to monitor the levels of these antibodies.
In addition, certain treatment medications may cause side effects that can be prevented or minimized by taking preventative measures. For example, rituximab – the mostly widely used monoclonal antibody to treat WM – can sometimes cause a rapid, short-term increase in IgM levels, called IgM flare. This increase in IgM can cause the blood to thicken, leading to hyperviscosity syndrome. Some people may need to have plasmapheresis before starting treatment with rituximab to reduce the risk of symptomatic hyperviscosity. It’s generally recommended that treatment with rituximab be withheld in people whose blood levels of IgM is greater than 4000mg/dL to minimize the risk of an IgM flare.
Another consideration is whether or not you might have a stem cell transplant as a future treatment. Some chemotherapy drugs are toxic to bone marrow stem cells from which new blood cells are made. Your doctor will limit the use of these drugs if a stem cell transplant is a possibility.
A long-term complication of some chemotherapy drugs – and the associated damage to stem cells – is the possibility of developing other types of blood disorders unrelated to WM, such as diffuse large B-cell lymphoma. However, this affects a very small percentage of people. It’s more common in people who receive alkylating agents or fludarabine (a nucleoside analog). While it’s important to recognize these possibilities, it does not mean these treatments shouldn’t be used. Discuss any concerns you have with your hematologist/oncologist, who will help you weigh the risks versus benefits of these particular agents.
What happens if the treatment doesn’t work well or the cancer comes back?
If the initial treatment regimen doesn’t work, another drug or set of drugs might give you better results. No single treatment for WM works for everyone with the disease.
Even if the initial therapy was successful getting the disease under control, the cancer may come back at some later time. This is called relapse. At this point, you and your hematologist/oncologist will discuss next steps, be it continued monitoring or re-treatment (sometimes called salvage therapy). Because WM is not curable and the disease grows slowly, nearly all people with WM will need treatment with different drugs at some point in time.
Your overall health condition, severity of symptoms, and quality of life will factor into the decision of when to begin re-treatment.
The choice of treatment after relapse depends on several things, including:
- The initial treatment used
- Your tolerance of the initial treatment
- The duration of response, meaning how soon did the cancer return after treatment?
- Your eligibility for a stem cell transplant
In general, if your WM remained under control for at least one year after initial treatment, repeat treatment with the same drug(s) can often get the cancer back under control. If the cancer returns sooner, or the prior treatment was not very effective, switching to a different therapy regimen is recommended. If you’re a candidate for a stem cell transplant, it’s important to avoid drugs that are toxic to stem cells, especially if you haven’t had any stem cells harvested.
Fortunately, there are many treatment choices for people who relapse and the options are continually increasing. You might also consider participating in a clinical trial. When weighing treatment options following relapse, it’s perfectly appropriate to get a second opinion from a WM expert.