The IWMF provides comprehensive information about the types of treatments used in the management of Waldenstrom macroglobulinemia (WM). Our Treatment Options Guides provide thorough descriptions about different categories of drug therapies, while our Fact Sheets provide detailed information about specific drugs and other treatments. Links to these IWMF publications are provided throughout the following overview.
What types of treatments and interventions are used in the management of Waldenstrom’s macroglobulinemia?
There are several types of treatments and interventions currently used to manage WM.
These interventions are not cancer treatments. They are used to relieve symptoms and, when needed, to help your body prepare for cancer treatment.
- Plasmapheresis: IgM is mainly found in plasma, the liquid part of blood. Plasmapheresis uses a machine to remove the plasma, which contains the abnormal IgM protein found in WM, from the other blood components. The plasma is removed through an intravenous (IV) line and then replaced with donated plasma and saline solution (a mixture of salt and water). People with symptomatic hyperviscosity should have this procedure done right away to relieve symptoms and limit organ damage. Additionally, people with an IgM level greater than 3,000 to 4,000 mg/dL should have this done before taking rituximab (Rituxan®).Another name for plasmapheresis is plasma exchange. See the Plasmapheresis Fact Sheet for detailed information about what to expect during this procedure.
- Transfusion: A red blood cell transfusion is sometimes given following plasmapheresis to replace blood loss that leads to anemia (low red blood cell count). Separate from plasmapheresis, a transfusion may be given if you’re experiencing severe symptomatic anemia. During a transfusion, donated blood is given to you through an IV.
- Splenectomy: This is the surgical removal of the spleen. It may benefit some people with WM who have painful enlargement of the spleen that didn’t respond to drug therapy, or have an enlarged spleen and severely low blood counts.
Treatment may start with a supportive intervention to control symptoms of the disease. However, supportive interventions do not treat the underlying cause of the symptoms, meaning the cancer cells themselves. Various types of drugs are used to treat the cancer cells. Cancer treatment for WM may consist of just one drug (single agent therapy), or two or more drugs (combination therapy). The drugs can be given in different combinations and schedules.
Many different types of drugs are used to treat cancer. They generally fall into one of the following categories: chemotherapy, targeted therapy, or corticosteroids. These drugs may be used as single agents or combined with other drugs and/or treatments.
- Chemotherapy: Also called chemo for short, this therapy works by killing, stopping, or slowing the growth of cancer cells.
Most chemotherapy drugs used to treat WM are given intravenously (IV). Some are given by injection or taken by mouth as a pill. Chemotherapy is usually given in cycles. Treatment days are followed by rest days, allowing your body to recover, before the next treatment cycle begins. This pattern often continues for several weeks to months. Most chemotherapy treatments are given on an outpatient basis – meaning you do not stay overnight – at a hospital, clinic, or doctor’s office.
To learn about the different types of chemotherapy medicines used to treat people with WM, click on the following links to our Treatment Options Guides and Fact Sheets:
-
- Treatment Guide: Alkylating Agents and Nucleoside Analogs
- Alkylating Agents
- cyclophosphamide (Cytoxan®)
- bendamustine (Treanda®)
- Nucleoside Analogs
- fludarabine (Fludara®),
- cladribine (2CdA or Leustatin®)
- Alkylating Agents
- Treatment Guide: Alkylating Agents and Nucleoside Analogs
- Targeted therapy: Researchers have identified specific features of cancer cells that are different from normal cells. This information is used to create targeted therapies that attack cancer cells without damaging normal cells, leading to fewer side effects. Each type of targeted therapy is a little different, but all interfere with the ability of a cancer cell to grow, divide, repair, die, or communicate with other cells. Many classes of drugs are considered targeted therapies. They are discussed in detail in the following Treatment Options Guides and Fact Sheets:
-
- Treatment Guide: Targeted Therapies and Pathway Inhibitors
- everolimus (Afinitor®)
- ibrutinib (Imbruvica®)
- acalabrutinib (Calquence®)
- zanubrutinib (Brukinsa®)
- Treatment Guide: Targeted Therapies and Pathway Inhibitors
-
- Treatment Guide: Monoclonal Antibodies
Antibodies are proteins made by your immune system to help fight infections. These drugs are man-made versions of antibodies that are designed to attack a specific target, such as a substance on the surface of B-lymphocytes, the cells where WM starts.
-
-
- rituximab (Rituxan®)
- ofatumumab (Arzerra®)
- Treatment Guide: Protease Inhibitors
-
Proteasomes are cellular complexes that maintain the right balance of proteins in cells by destroying unneeded proteins. Protease inhibitors stop proteasomes from breaking down excess proteins. When proteins in cancer cells build up, the cells eventually die.
-
-
- bortezomib (Velcade®)
- carfilzomib (Kyprolis®)
- ixazomib (Ninlaro®)
-
- Corticosteroids: Also called steroids for short, these drugs are usually used to relieve inflammation, but some also have anti-cancer effects. They’re frequently used in combination with other therapies or as pre-treatments to help prevent allergic reactions to other drugs being administered. Steroids are often included as part of chemotherapy regimens. The most common corticosteroids used in WM treatment are dexamethasone (Decadron®), prednisolone, and prednisone.
Blood stem cells are cells that develop into mature blood cells. Stem cells and mature blood cells are made in bone marrow. The goal of a stem cell transplant (SCT) is to replace unhealthy blood stem cells with healthy ones. Stem cell transplant is not used for people newly diagnosed with WM. It may be an option for treating WM that returns after initial treatment, called relapsed WM.
If there’s a possibility you might have a SCT in the future, there are certain chemotherapy medicines that should be avoided during initial treatment because they are toxic to bone marrow stem cells. Talk to your doctor about your eligibility and possible need for a SCT as a future treatment.
There are two types of stem cell transplantation:
-
- Allogenic: The stem cells for transplant come from a donor.
- Autologous: Your own stem cells are used for transplant.
An autologous SCT has less risks and side effects, and is the type most often used to treat people with WM.
-
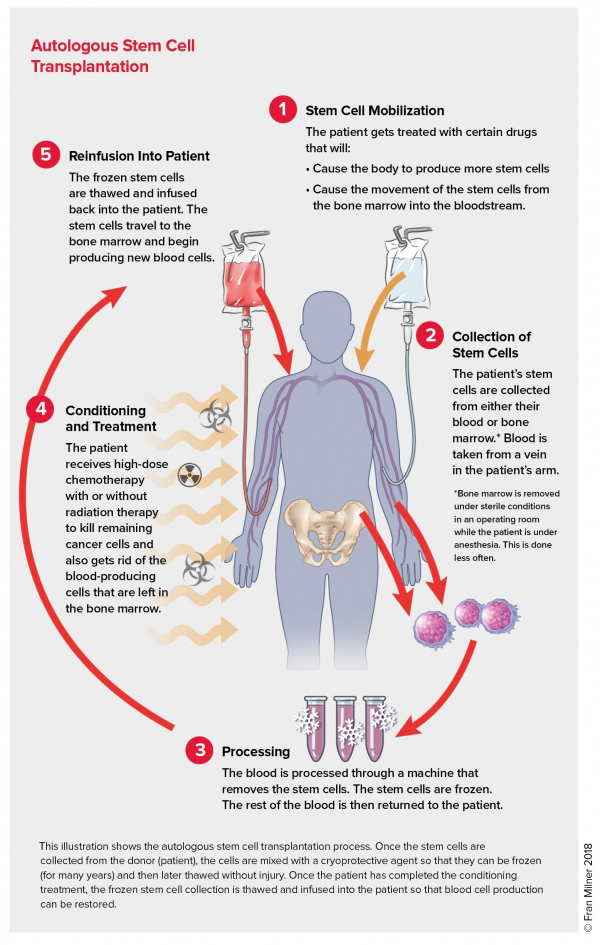
- Autologous Stem Cell Transplant: Blood-forming stem cells are made in the bone marrow, but can also be found in blood. In an autologous SCT, the stem cells are usually taken from your blood. Because there aren’t many stem cells naturally found in blood, you’ll be given a medicine (by injection) for five to six days that increases the number of stem cells your body makes. Following this, the stem cells are removed from your blood by a machine, and then frozen and stored until the transplant.
After your stem cells have been collected, you’ll receive high-dose chemotherapy, with or without radiation, to kill the cancerous WM cells in your bone marrow. However, these high dose treatments are toxic to normal cells in bone marrow as well, accounting for the side effects and complications that can occur with SCT. Destroying normal bone marrow cells increases the risk of:
-
-
- Infection, due to decreased white blood cells.
- Bleeding, due to decreased platelets.
- Fatigue, due to decreased red blood cells (anemia).
-
During this time, your immune system is very weak and extra precautions must be taken to avoid infection. You’ll need to stay in a special hospital room where a sterile environment can be maintained. You may also get antibiotics to prevent infection, and blood transfusions to prevent bleeding and anemia.
When chemotherapy is finished, your frozen stem cells are thawed and put back into your body using a transfusion. The transplanted stem cells travel to your bone marrow and grow, forming new healthy blood cells. This process, called engraftment, takes about two to four weeks.
While the risks of stem cell transplant have decreased over the decades, it is a demanding procedure that can be hard on your body. SCT often requires a long hospital stay and can cause life-threatening side effects due to the high doses of chemotherapy used. Your doctor will order a number of tests to make sure you are healthy enough to undergo SCT. If you are advanced in age, or have major health problems such as heart, lung, or kidney disease, you may not be a good candidate for SCT.
For some people with WM, participation in a clinical trial may be the best (or only) treatment option.
Clinical trials are research studies, conducted under strict guidelines, to help researchers determine the beneficial effects and possible adverse effects of new treatments. Studies are also conducted to evaluate new uses for therapies that have been approved for other cancers or types of disease. Patient participation in clinical trials is important in the development of new and more effective treatments for WM. Participating in a trial may provide you, and ultimately other people with WM, access to the latest and most promising treatments available. For more information, refer to our clinical trials section.